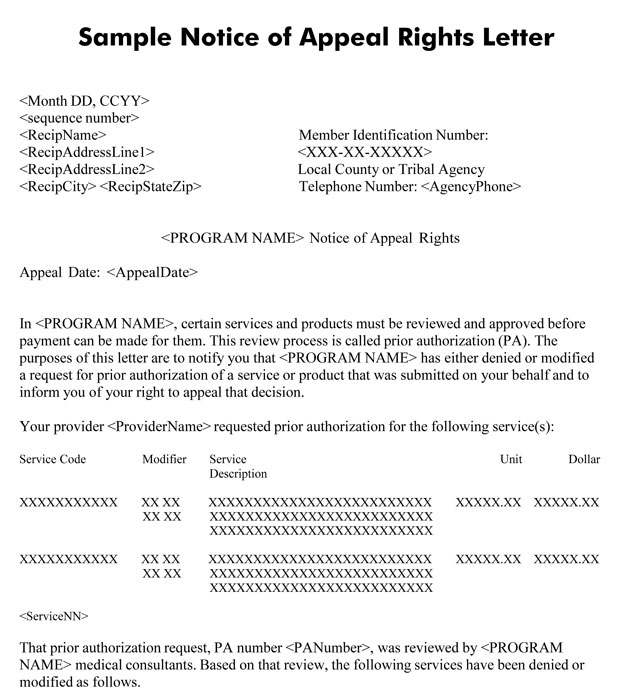
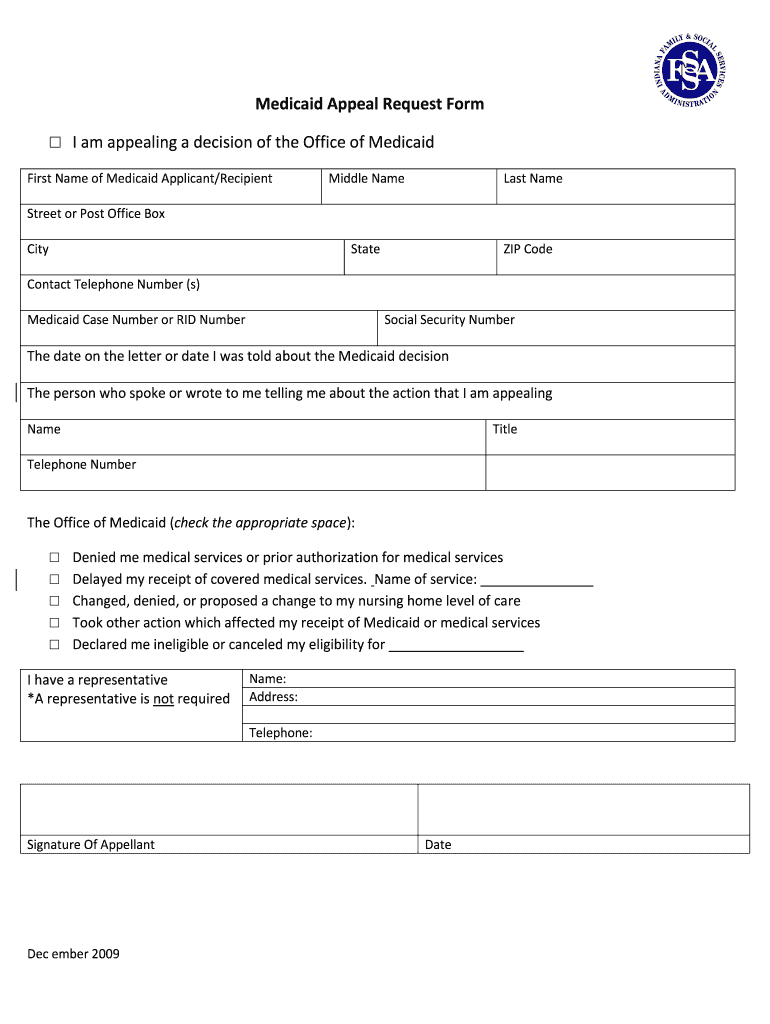
Medicaid Texas Appeal Form - Web the prior authorization reconsideration request form is required to initiate a request for reconsideration of a previously denied. Providers may use three methods to appeal. Web form 8608, sample appeal letter instructions for opening a form some forms cannot be viewed in a web browser and must be. You can call member services at: Web form 3094, application for program benefits: Web attestation form for collaborative care model (cocm) in texas medicaid (112.42 kb) 12/7/2022; *is this a request for reconsideration: Tell us about the complaint or appeal. Providers may use three methods. You have 2 ways to tell us your complaint:
Amerigroup Appeal Form Fill Out and Sign Printable PDF Template signNow
Web attestation form for collaborative care model (cocm) in texas medicaid (112.42 kb) 12/7/2022; You can call member services at: Community first cocm provider attestation form. Web provider appeals to hhsc medical and ur appeals. Web member services staff can help you file an appeal.
Medicaid Appeal Form Wisconsin Form Resume Examples
Web provider appeals to hhsc medical and ur appeals. To submit an appeal on paper, mail or fax the appeal to. A written appeal request with all required documentation must be received. Web form 3094, application for program benefits: Web please complete the following form to help expedite the review of your claims appeal.

TX BCBS Physician/Professional Provider & Facility Ancillary Request
Web form 3094, application for program benefits: You have 2 ways to tell us your complaint: Web claim inquiry/appeal form claim inquiry/appeal form instructions for filing a claim inquiry or appeal: Web medicaid prior authorization forms inpatient medicaid authorization form (pdf) outpatient medicaid authorization form. Web the prior authorization reconsideration request form is required to initiate a request for reconsideration.
8 Texas Medicaid Forms And Templates free to download in PDF
Web the prior authorization reconsideration request form is required to initiate a request for reconsideration of a previously denied. Web an appeal is a request for reconsideration of a previously dispositioned claim. Web member services staff can help you file an appeal. Providers may use three methods to appeal. You have 2 ways to tell us your complaint:

Molina Healthcare Prescription Drug Prior Authorization Request Form
Please describe the issue in as. Providers may use three methods. Fill out this form completely. Tell us about the complaint or appeal. To submit an appeal on paper, mail or fax the appeal to.
Check your health plan documents or contact your health plan or employer for details on your plan’s. Web the prior authorization reconsideration request form is required to initiate a request for reconsideration of a previously denied. To submit an appeal on paper, mail or fax the appeal to. Web member services staff can help you file an appeal. Web provider.
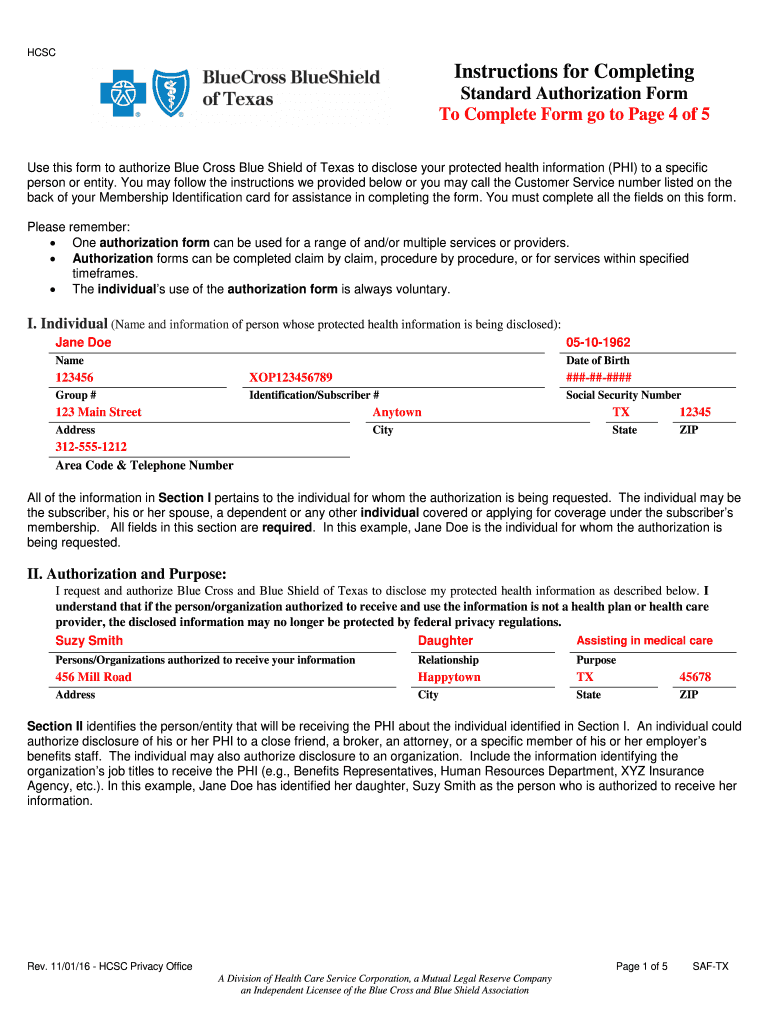
2012 Form TX Blue Cross Blue Shield SAFTX Fill Online, Printable
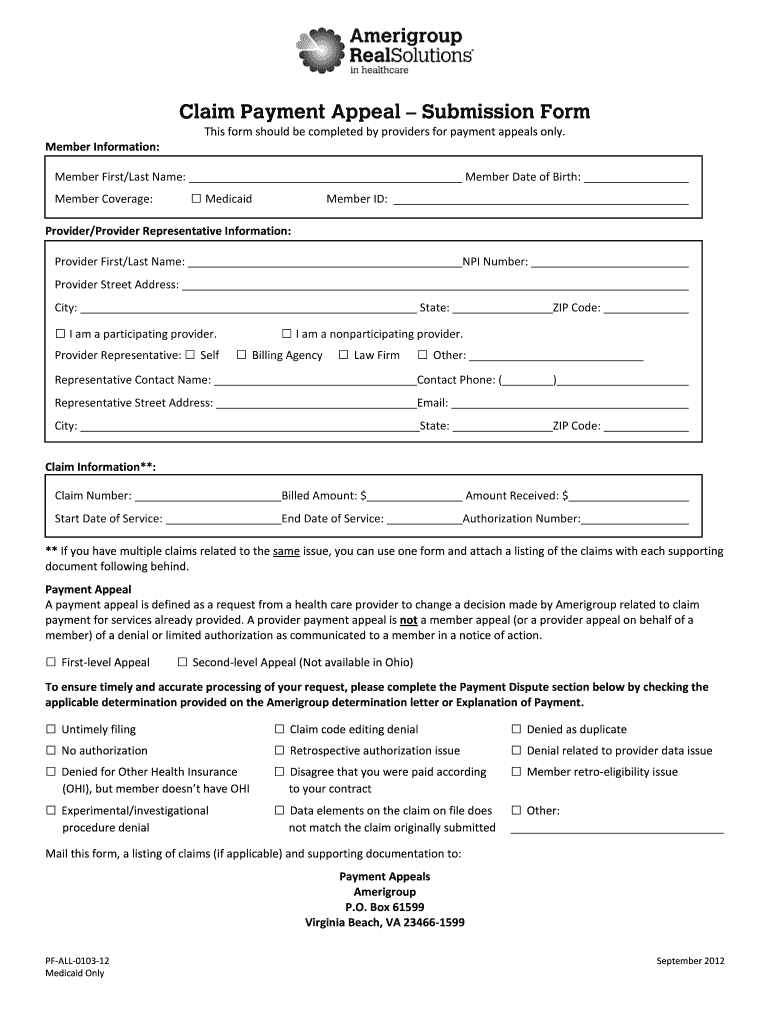
Web provider appeal request form • please complete one form per member to request an appeal of an adjudicated/paid claim. *is this a request for reconsideration: Web how to file an appeal: Web a claim appeal form must be sent in with an appeal submitted on paper. Web the prior authorization reconsideration request form is required to initiate a request.

Texas Medicaid Application Form Download Form Resume Examples
To submit an appeal on paper, mail or fax the appeal to. Web form 8608, sample appeal letter instructions for opening a form some forms cannot be viewed in a web browser and must be. Web form 3094, application for program benefits: Providers may use three methods. Web provider appeal request form • please complete one form per member to.
Indiana Medicaid Appeal Form Fill Online, Printable, Fillable, Blank
Web provider appeals to hhsc medical and ur appeals. You have 2 ways to tell us your complaint: Web please complete the following form to help expedite the review of your claims appeal. Web form 3094, application for program benefits: Web a claim appeal form must be sent in with an appeal submitted on paper.

Texas appeals court allows 350M in Medicaid therapy cuts WOAI
To submit an appeal on paper, mail or fax the appeal to. Web member services staff can help you file an appeal. Web medicaid members will have sixty (60) calendar days from the date of superior’s notice of adverse benefit determination. Web how to file a complaint. Web provider appeal request form • please complete one form per member to.
Providers may use three methods. Fill out this form completely. Option care women's health referral form. Web an appeal is a request for reconsideration of a previously dispositioned claim. Web form 8608, sample appeal letter instructions for opening a form some forms cannot be viewed in a web browser and must be. You have 2 ways to tell us your complaint: To submit an appeal on paper, mail or fax the appeal to. Providers may use three methods to appeal. Web a claim appeal form must be sent in with an appeal submitted on paper. Web an appeal is a request for reconsideration of a previously dispositioned claim. Web the prior authorization reconsideration request form is required to initiate a request for reconsideration of a previously denied. A written appeal request with all required documentation must be received. You can call member services at: Web form 3094, application for program benefits: Web attestation form for collaborative care model (cocm) in texas medicaid (112.42 kb) 12/7/2022; Please describe the issue in as. Web provider appeals to hhsc medical and ur appeals. Web how to file an appeal: Tell us about the complaint or appeal. Web medicaid members will have sixty (60) calendar days from the date of superior’s notice of adverse benefit determination.
To Submit An Appeal On Paper, Mail Or Fax The Appeal To.
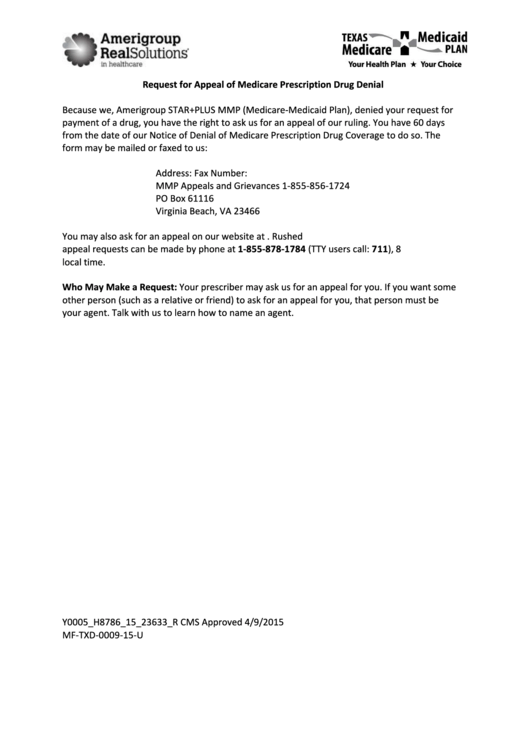
Fill out this form completely. Web form 8608, sample appeal letter instructions for opening a form some forms cannot be viewed in a web browser and must be. If you are asking for a standard appeal or a fast appeal, make your appeal in writing or call. Web a claim appeal form must be sent in with an appeal submitted on paper.
Web An Appeal Is A Request For Reconsideration Of A Previously Dispositioned Claim.
You may use this form if you would like to write to us: Web please complete the following form to help expedite the review of your claims appeal. Web medicaid prior authorization forms inpatient medicaid authorization form (pdf) outpatient medicaid authorization form. Web how to file an appeal:
Community First Cocm Provider Attestation Form.
Web how to file a complaint. Providers may use three methods. You have 2 ways to tell us your complaint: A written appeal request with all required documentation must be received.
Web Provider Appeal Request Form • Please Complete One Form Per Member To Request An Appeal Of An Adjudicated/Paid Claim.
Web member services staff can help you file an appeal. Web claim inquiry/appeal form claim inquiry/appeal form instructions for filing a claim inquiry or appeal: Web i want to report a complaint or appeal. Check your health plan documents or contact your health plan or employer for details on your plan’s.