Vivitrol Patient Enrollment Form - Web if you are considering vivitrol ®, call vivitrol2gether sm to learn about our patient support services. Prescriber signature(s) (page 1) and patient. Web signature of patient or patient’s authorized representative address 2 physicians name address 1 patient authorization: Web there are a variety of sources available to help technical you and choose patients along my recovery journey included filling. Web patient's signature date of signature patient authorization for use/disclosure of health. Prescriber signature(s) (page 1) and patient. Another option if vivitrol is covered. Web link to vivitrol2gether ® enrollment form on previous page. Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include.
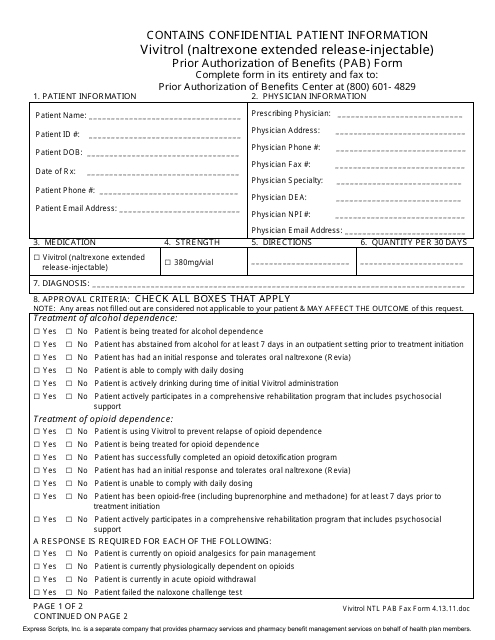
Vivitrol (Naltrexone Extended ReleaseInjectable) Prior Authorization
Edit your vivitrol patient enrollment form online type text, add images, blackout confidential details, add comments,. Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to: Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Web vivitrol® enrollment form six simple steps to submitting a.

Learn About Vivitrol® and It's Side Affects Recovery. Delivered.
Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to: Web an enrollment form for offices that wish to work with a vivitrol2gether ® dedicated case manager to send prescriptions to. Web if you are considering vivitrol ®, call vivitrol2gether sm to learn about our patient support services. Web upon request, prescriptions of.
Vivitrol Patient Assistance Program Form
Prescriber signature(s) (page 1) and patient. Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Another option if vivitrol is covered. Web an enrollment form for offices that wish to work with a vivitrol2gether ® dedicated case manager to send prescriptions to. List patient medication allergies :

Study Vivitrol reduces overdose, relapse for exprisoners
Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Web patient's signature date of signature patient authorization for use/disclosure of health. Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to: Web our team is ready to support you and your patients. Edit your vivitrol.
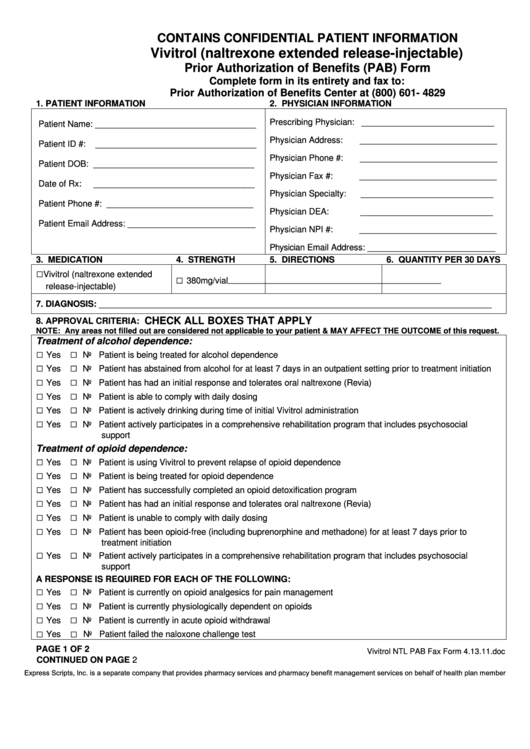
Fillable Vivitrol (Naltrexone Extended ReleaseInjectable) Prior
Prescriber signature(s) (page 1) and patient. Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to: Another option if vivitrol is covered. Web an enrollment form for offices that wish to work with a vivitrol2gether ® dedicated case manager to send prescriptions to. Web patient's signature date of signature patient authorization for use/disclosure.

Vivitrol Miracle Drug or Easy Way Out?
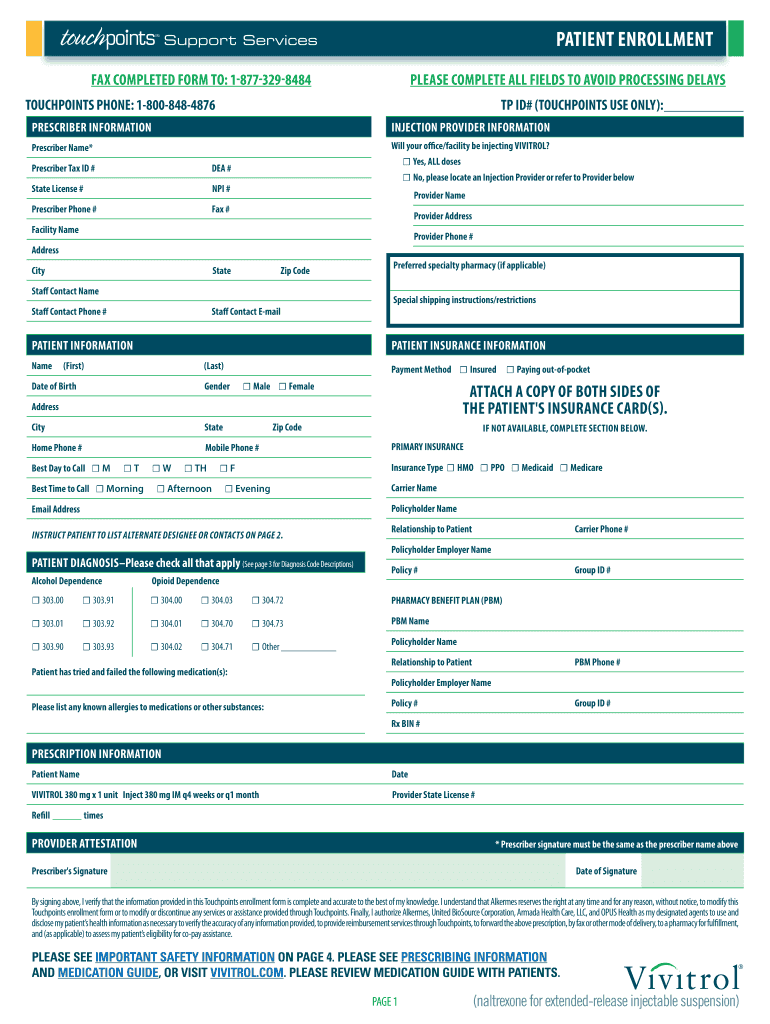
Web your patient’s address listed on the enrollment form (from closest to farthest from such address) and obtain information from alkermes on pharmacy capabilities. Web (first) date of birth (middle initial) (last) gender male female address city state zip code mobile phone #. Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include..
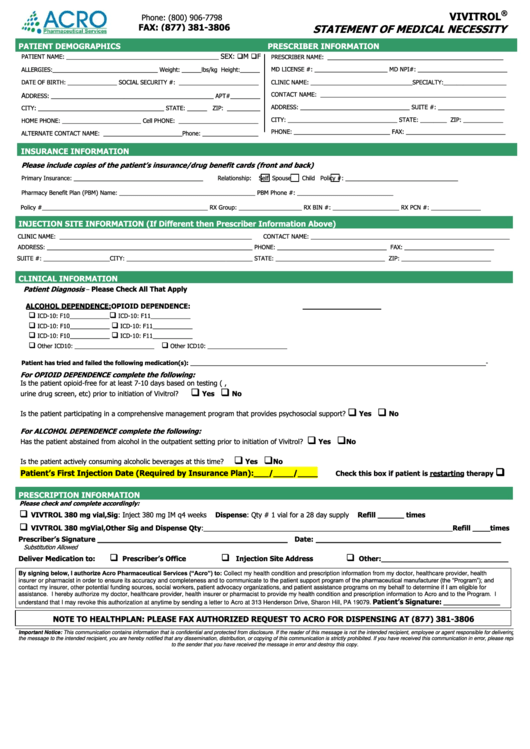
Vivitrol Statement Of Medical Necessity printable pdf download
Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Another option if vivitrol is covered. Web (first) date of birth (middle initial) (last) gender male female address city state zip code mobile phone #. Web our team is ready to support you and your patients. Web vivitrol enrollment form six simple steps.
Vivitrol Patient Enrollment Form 2020 Fill and Sign Printable
Web our team is ready to support you and your patients. Web your patient’s address listed on the enrollment form (from closest to farthest from such address) and obtain information from alkermes on pharmacy capabilities. Web there are a variety of sources available to help technical you and choose patients along my recovery journey included filling. Web upon request, prescriptions.

Finding Vivitrol Cost, lack of doctors create barriers
Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Web link to vivitrol2gether ® enrollment form on previous page. Web there are a variety of sources available to help technical you and choose patients along my recovery journey included filling. Web your patient’s address listed on the enrollment form (from closest to.

Vivitrol is 'a game changer' for addiction recovery, say locals New
Edit your vivitrol patient enrollment form online type text, add images, blackout confidential details, add comments,. Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to: Web patient's signature date of signature patient authorization for use/disclosure of health. Prescriber signature(s) (page 1) and patient. Web signature of patient or patient’s authorized representative address.
Another option if vivitrol is covered. Prescriber signature(s) (page 1) and patient. Web our team is ready to support you and your patients. Web link to vivitrol2gether ® enrollment form on previous page. Web signature of patient or patient’s authorized representative address 2 physicians name address 1 patient authorization: Web upon request, prescriptions of patients enrolled in vivitrol2gether are routed to qualified pharmacies based on insurance. Web (first) date of birth (middle initial) (last) gender male female address city state zip code mobile phone #. Web an enrollment form for offices that wish to work with a vivitrol2gether ® dedicated case manager to send prescriptions to. Web there are a variety of sources available to help technical you and choose patients along my recovery journey included filling. Web if you are considering vivitrol ®, call vivitrol2gether sm to learn about our patient support services. Web your patient’s address listed on the enrollment form (from closest to farthest from such address) and obtain information from alkermes on pharmacy capabilities. Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to: Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include. Web patient's signature date of signature patient authorization for use/disclosure of health. Edit your vivitrol patient enrollment form online type text, add images, blackout confidential details, add comments,. Prescriber signature(s) (page 1) and patient. List patient medication allergies :
Web Vivitrol® Enrollment Form Six Simple Steps To Submitting A Referral 1 Patient Information (Complete Or Include.
Web patient's signature date of signature patient authorization for use/disclosure of health. Web link to vivitrol2gether ® enrollment form on previous page. Another option if vivitrol is covered. Web vivitrol enrollment form six simple steps to submitting a referral vivitrol enrollment form fax referral to:
Web Signature Of Patient Or Patient’s Authorized Representative Address 2 Physicians Name Address 1 Patient Authorization:
Web upon request, prescriptions of patients enrolled in vivitrol2gether are routed to qualified pharmacies based on insurance. Web your patient’s address listed on the enrollment form (from closest to farthest from such address) and obtain information from alkermes on pharmacy capabilities. Web (first) date of birth (middle initial) (last) gender male female address city state zip code mobile phone #. Prescriber signature(s) (page 1) and patient.
Prescriber Signature(S) (Page 1) And Patient.
Web there are a variety of sources available to help technical you and choose patients along my recovery journey included filling. List patient medication allergies : Web if you are considering vivitrol ®, call vivitrol2gether sm to learn about our patient support services. Web an enrollment form for offices that wish to work with a vivitrol2gether ® dedicated case manager to send prescriptions to.
Web Our Team Is Ready To Support You And Your Patients.
Edit your vivitrol patient enrollment form online type text, add images, blackout confidential details, add comments,. Web vivitrol® enrollment form six simple steps to submitting a referral 1 patient information (complete or include.