Metroplus Authorization Request Form - Web follow the simple instructions below: Web please use this universal aba request form for initial requests for assessment, as well as initial and concurrent treatment plan. Covermymeds is metroplus prior authorization forms’s preferred method. _____ *please attach the most recent clinical notes or supporting documentation* metroplus. Please ensure completion of this form in its entirety and. Metroplus health plan plan phone no. Web metroplushealth is a health insurance provider that offers provider authorization for its members. Web nys medicaid prior authorization request form for prescriptions plan name: Web managed long term care plan prior authorization request form 160 water street, 3rd floor new york, ny 10038 (855) 355. Web metroplus authorization request patient information:
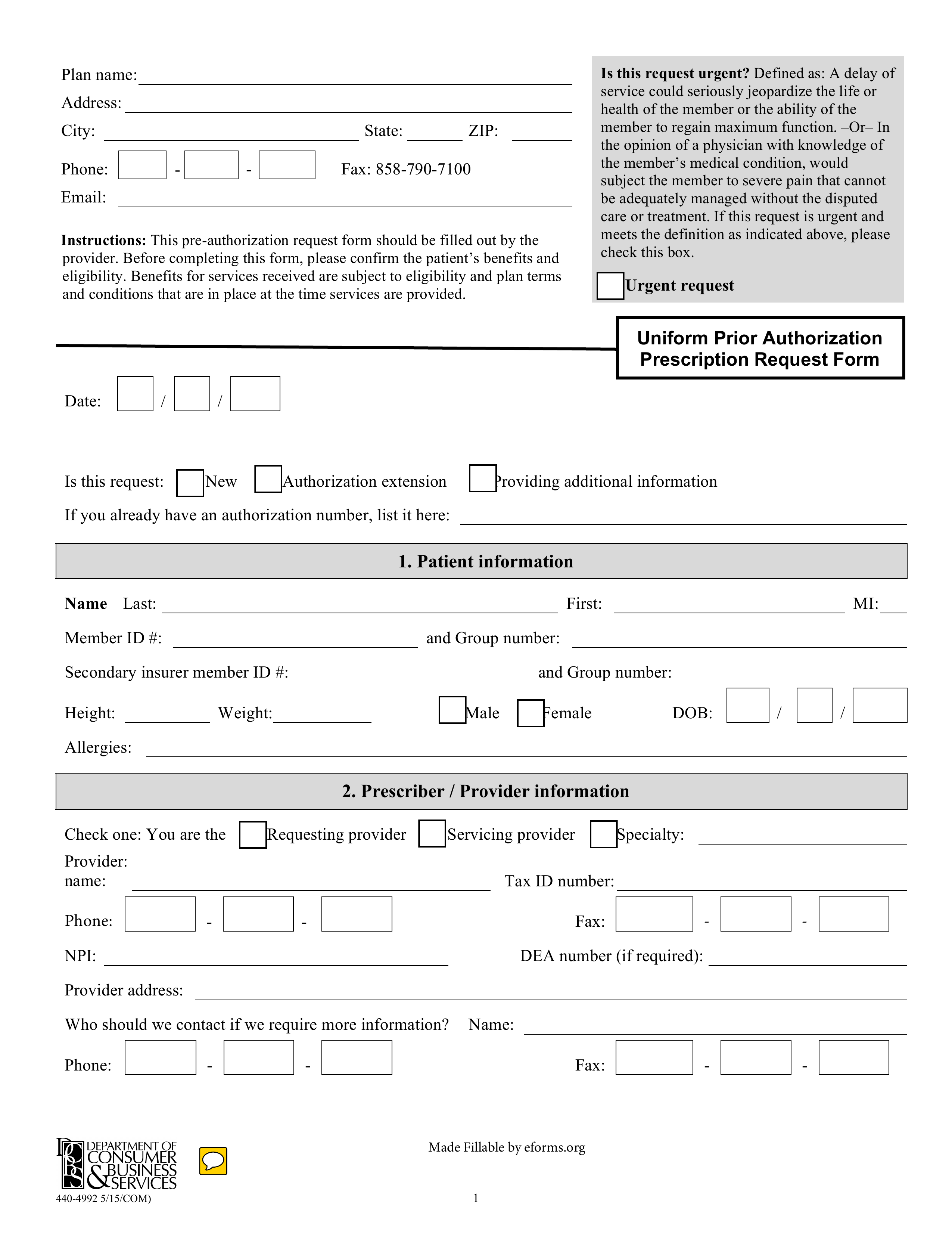
Free Medicare Prior Rx Authorization Form Pdf Eforms
Please ensure completion of this form in its entirety and. Have you been trying to find a fast and efficient tool to fill in metroplus authorization. Web metroplushealth is a health plan for new york city employees that offers various provider forms for providers to. Web nys medicaid prior authorization request form for prescriptions plan name: Metroplus health plan plan.
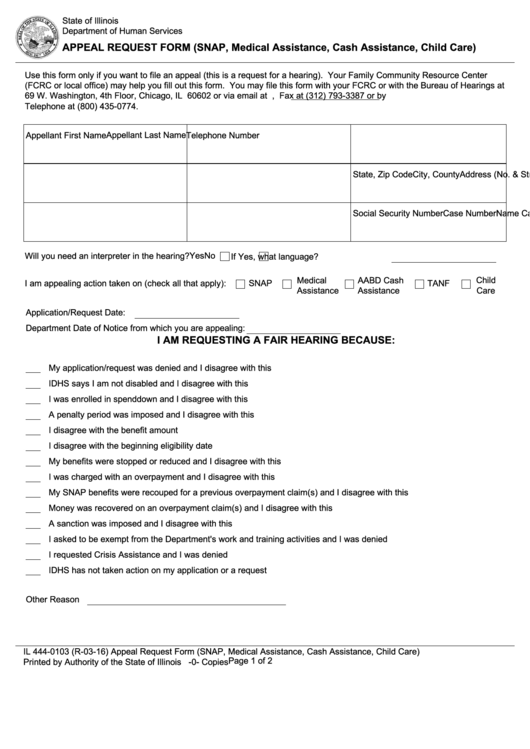
Fillable Appeal Request Form printable pdf download
Web nys medicaid prior authorization request form for prescriptions plan name: Metroplus health plan plan phone no:. Metroplus health plan plan phone no. Please ensure completion of this form in its entirety and. Web metroplushealth is a health insurance provider that offers provider authorization for its members.
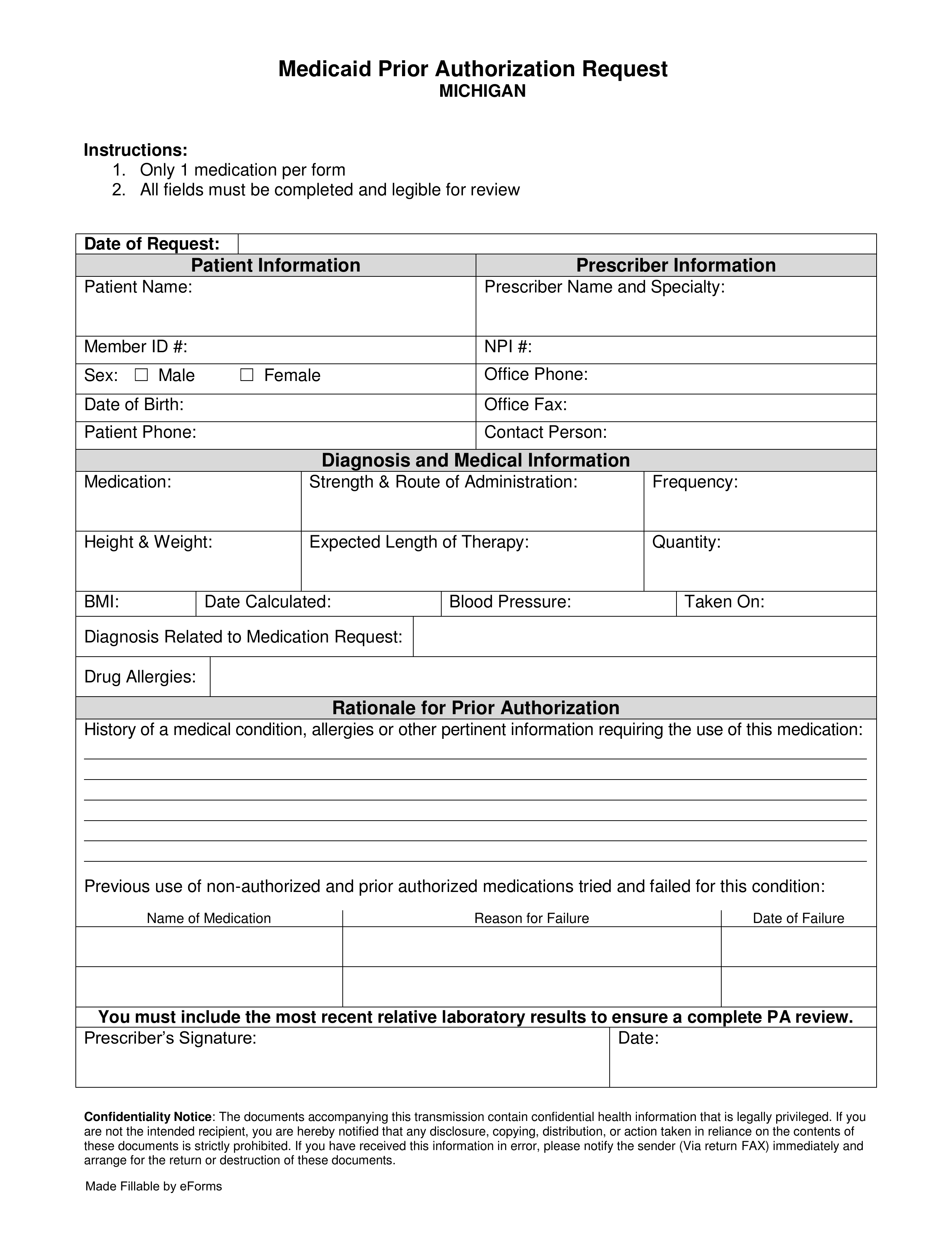
Free Michigan Medicaid Prior (Rx) Authorization Form PDF eForms
Web follow the simple instructions below: Web nys medicaid prior authorization request form for prescriptions plan name: Metroplus health plan plan phone no. Web this notice describes how medical information about you may be used and disclosed and how you can get access. Metroplus health plan plan phone no:.

University Family Care Prior Auth Form Fill Online, Printable
Metroplus health plan plan phone no. Web this notice describes how medical information about you may be used and disclosed and how you can get access. Web this form is to be filled out in its entirety for all requests; Web this form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized.

Metroplus Authorization Request Form
Web metroplus authorization request patient information: _____ *please attach the most recent clinical notes or supporting documentation* metroplus. Edit your m11q form metroplus online type text, add images, blackout confidential details, add comments, highlights and. Web this form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. You will be notified.

Automate healthcare gov marketplace appeals appeal forms airSlate
Web please use this universal aba request form for initial requests for assessment, as well as initial and concurrent treatment plan. You will be notified of the service. Covermymeds is metroplus prior authorization forms’s preferred method. Web select the appropriate metroplus form to get started. Metroplus health plan plan phone no.
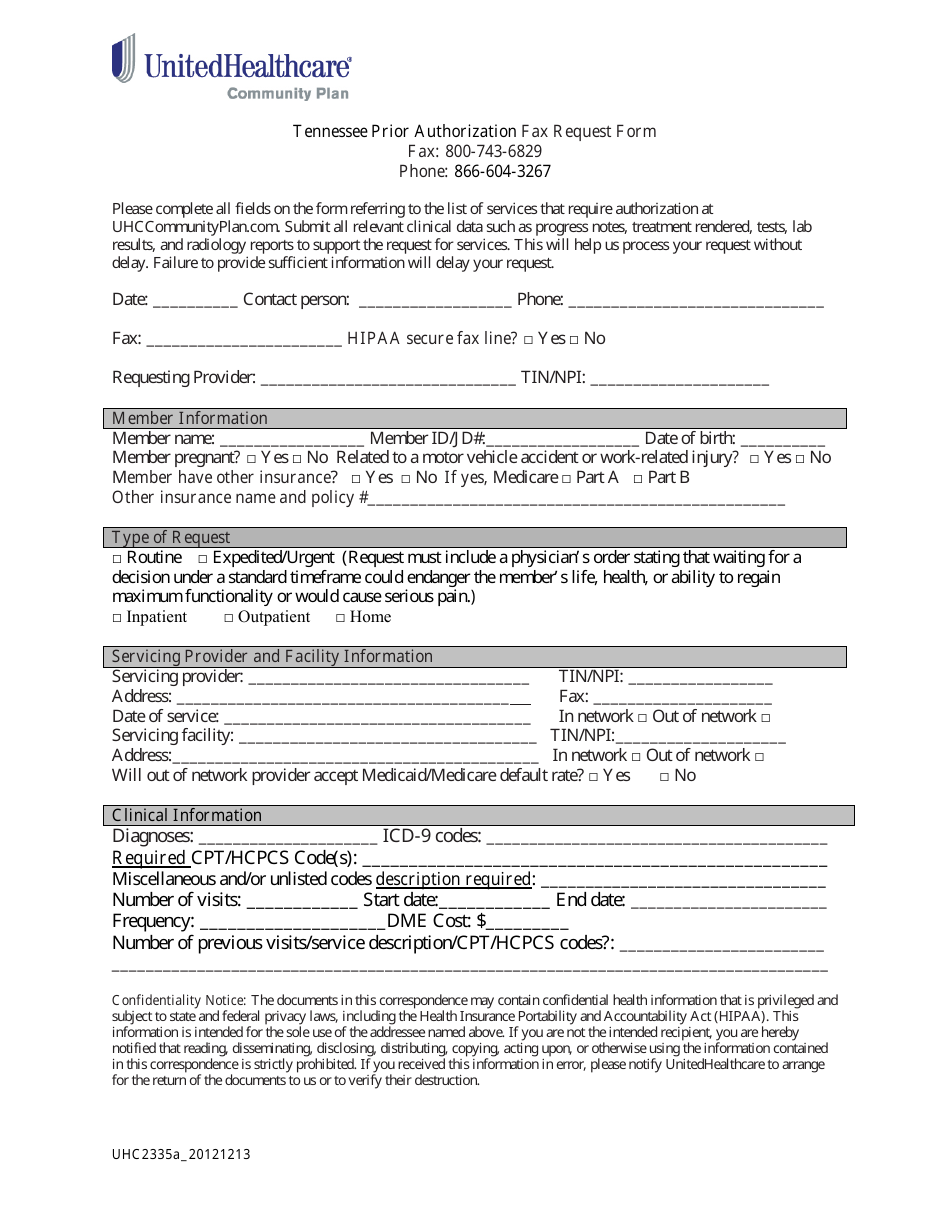
Tennessee Tennessee Prior Authorization Fax Request Form
Please ensure completion of this form in its entirety and. Web please use this universal aba request form for initial requests for assessment, as well as initial and concurrent treatment plan. Web nys medicaid prior authorization request form for prescriptions plan name: Web date form completed and faxed: Covermymeds is metroplus prior authorization forms’s preferred method.

Metroplus Authorization Request Form
Web follow the simple instructions below: Web this form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Covermymeds is metroplus prior authorization forms’s preferred method. _____ *please attach the most recent clinical notes or supporting documentation* metroplus. Web metroplus authorization request patient information:
FREE 35+ Sample Authorization Forms in PDF
Web follow the simple instructions below: Web metroplushealth is a health insurance provider that offers provider authorization for its members. Web nys medicaid prior authorization request form for prescriptions plan name: Metroplus health plan plan phone no. You will be notified of the service.
Formulary ExceptionPrior Authorization Request Form Fill Out and Sign
Web metroplushealth is a health insurance provider that offers provider authorization for its members. Web use our provider authorization grid for medical services below to determine what prior authorization requirements are. Please ensure completion of this form in its entirety and. Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate. Have.
Please ensure completion of this form in its entirety and. Covermymeds is metroplus prior authorization forms’s preferred method. Web this notice describes how medical information about you may be used and disclosed and how you can get access. Web managed long term care plan prior authorization request form 160 water street, 3rd floor new york, ny 10038 (855) 355. Web date form completed and faxed: Edit your m11q form metroplus online type text, add images, blackout confidential details, add comments, highlights and. Metroplus health plan pharmacy utilization management department 50. Web select the appropriate metroplus form to get started. Web prior authorization request form fax: Metroplus health plan plan phone no:. Web metroplushealth is a health plan for new york city employees that offers various provider forms for providers to. Web stick to these simple steps to get metroplus health plan authorization request form prepared for submitting: Web metroplus authorization request patient information: Web please use this universal aba request form for initial requests for assessment, as well as initial and concurrent treatment plan. Web this form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. You will be notified of the service. Web follow the simple instructions below: Metroplus health plan plan phone no. Web use our provider authorization grid for medical services below to determine what prior authorization requirements are. _____ *please attach the most recent clinical notes or supporting documentation* metroplus.
Web Nys Medicaid Prior Authorization Request Form For Prescriptions Plan Name:
Web please use this universal aba request form for initial requests for assessment, as well as initial and concurrent treatment plan. _____ *please attach the most recent clinical notes or supporting documentation* metroplus. Web managed long term care plan prior authorization request form 160 water street, 3rd floor new york, ny 10038 (855) 355. Web this notice describes how medical information about you may be used and disclosed and how you can get access.
Web Select The Appropriate Metroplus Form To Get Started.
Web metroplus authorization request patient information: Metroplus health plan pharmacy utilization management department 50. Web follow the simple instructions below: Web stick to these simple steps to get metroplus health plan authorization request form prepared for submitting:
Web Date Form Completed And Faxed:
Edit your m11q form metroplus online type text, add images, blackout confidential details, add comments, highlights and. Metroplus health plan plan phone no:. Web metroplushealth is a health plan for new york city employees that offers various provider forms for providers to. Metroplus health plan plan phone no.
Web Prior Authorization Request Form Fax:
Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate. Web metroplushealth is a health insurance provider that offers provider authorization for its members. Web this form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Please ensure completion of this form in its entirety and.