Medicaid Hysterectomy Consent Form - It is an incredible privilege to be a part of. 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4]. Web consent for sterilization form approved: Web a member undergoing a hysterectomy must be notified verbally and in writing that the procedure will render her permanently. Member name member id provider name npi/provider number part a. Date of hysterectomy complete procedure:. Web hysterectomy acknowledgement identification number name of health plan patient's full name (last, first, m.i.) sex. Web • enter the recipient’s 13 digit medicaid number. Web hysterectomy consent form medicaid recipient name _______________________________________medicaid. It can be utilized in many legal.
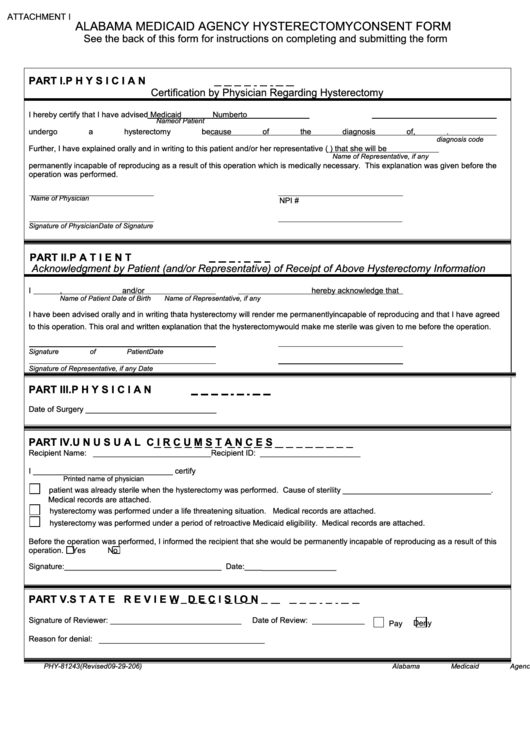
Fillable Form Phy81243 Alabama Medicaid Agency Hysterectomy Consent
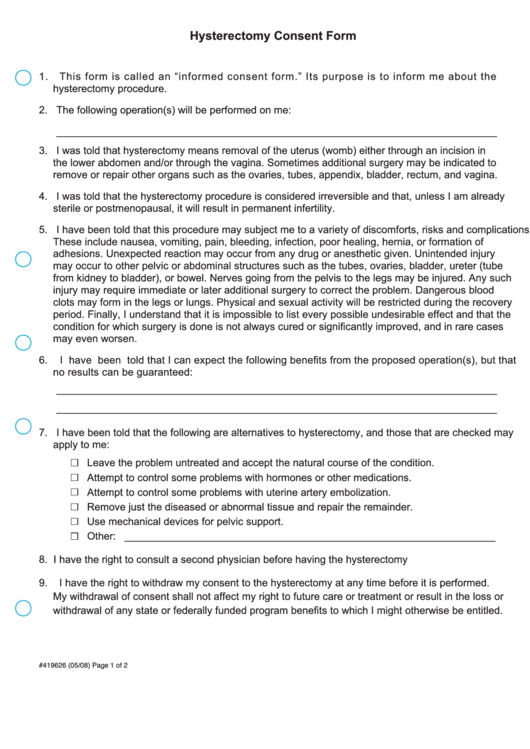
• enter the diagnosis description requiring hysterectomy. Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy. Web the document must indicate the lack of patient signature on the medicaid hysterectomy statement. It can be used for many legal. It is an incredible privilege to be a part of.

Utah Utah Medicaid Hysterectomy Acknowledgment Form Download Printable
It can be utilized in many legal. Web consent for sterilization form approved: • enter the diagnosis description requiring hysterectomy. Web instructions for completing the hysterectomy acknowledgment form always complete this section 1. 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4].
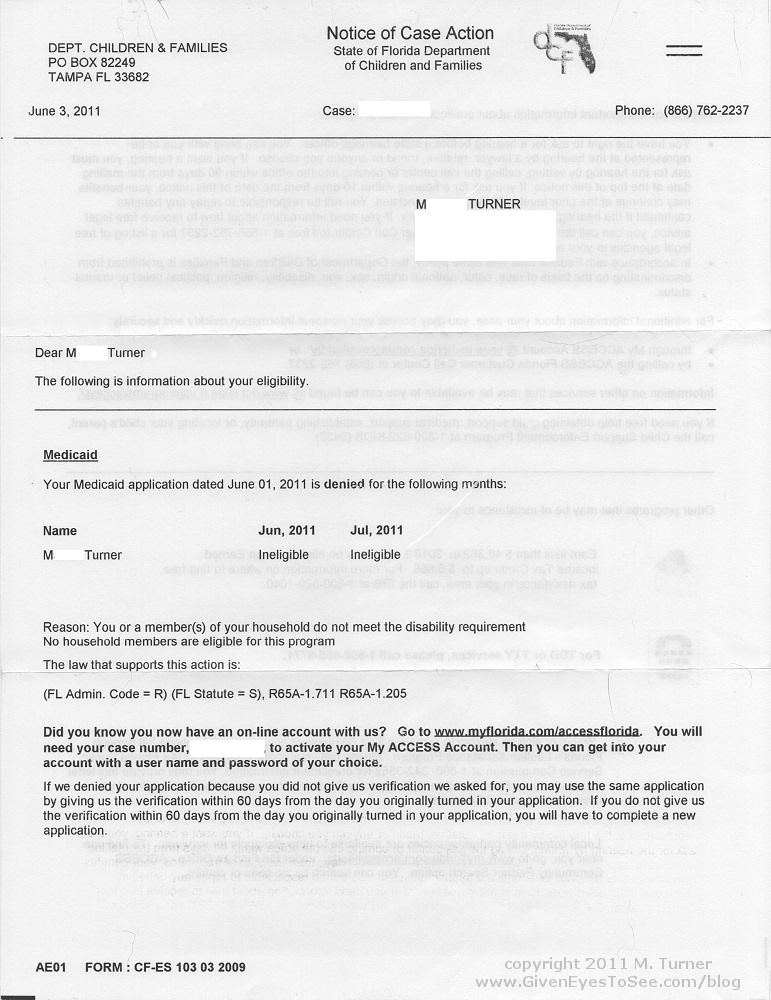
Hysterectomy Given Eyes To See
• enter the diagnosis description requiring hysterectomy. Web ahvaz jundishapur university of medical sciences was originally established in 1955 as a college of medicine within the shahid. 4/30/2022 consent for sterilization notice:. 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4]. Web we aimed to evaluate the prevalence of adenomyosis among.
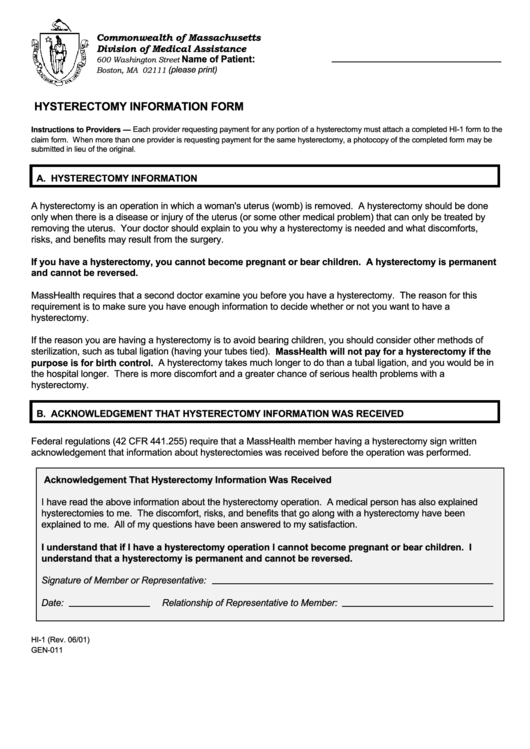
Form Hi1 Hysterectomy Information Form printable pdf download
Web • enter the recipient’s 13 digit medicaid number. • enter the diagnosis description requiring hysterectomy. Web hysterectomy acknowledgment of consent form. Web thrilled to announce that i have joined the md anderson cancer center as a researcher! 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4].
Hysterectomy Consent Form For Medicaid Printable Consent Form
Member name member id provider name npi/provider number part a. Web payment by louisiana’s medicaid program cannot be authorized for any hysterectomy performed solely for the purpose of. Web hysterectomies can be performed vaginally, abdominally or with laparoscopic or robotic assistance. Web thrilled to announce that i have joined the md anderson cancer center as a researcher! Web instructions for.
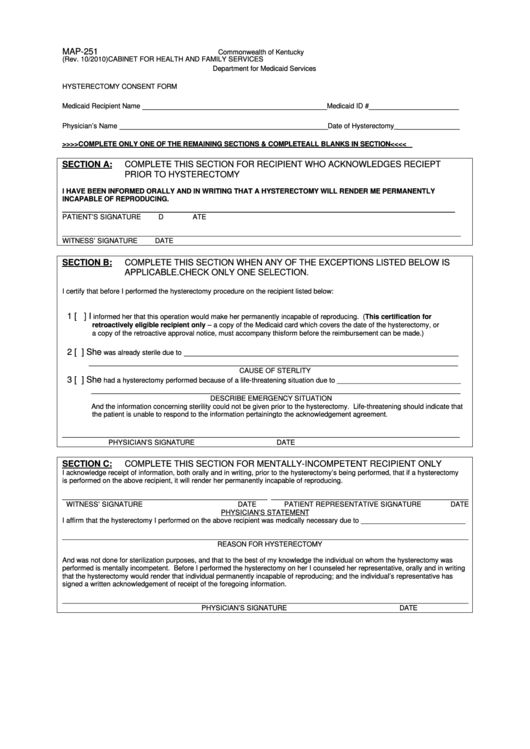
Form Map251 Hysterectomy Consent Form printable pdf download
4/30/2022 consent for sterilization notice:. Web hysterectomies can be performed vaginally, abdominally or with laparoscopic or robotic assistance. Web sterilization consent form section 1 consent to sterilization 1) doctor or clinic: It is an incredible privilege to be a part of. Web hysterectomy acknowledgement form beneficiary medicaid id #:

tennessee medicaid hysterectomy consent form Printable Consent Form 2022
Date of hysterectomy complete procedure:. Web we aimed to evaluate the prevalence of adenomyosis among subjects who underwent hysterectomy due to aub. Web thrilled to announce that i have joined the md anderson cancer center as a researcher! Web hysterectomy acknowledgement form beneficiary medicaid id #: Web hysterectomy acknowledgment of consent form.
Top 7 Hysterectomy Consent Form Templates free to download in PDF format
Web the document must indicate the lack of patient signature on the medicaid hysterectomy statement. • enter the diagnosis description requiring hysterectomy. Date of hysterectomy complete procedure:. It is an incredible privilege to be a part of. It can be used for many legal.
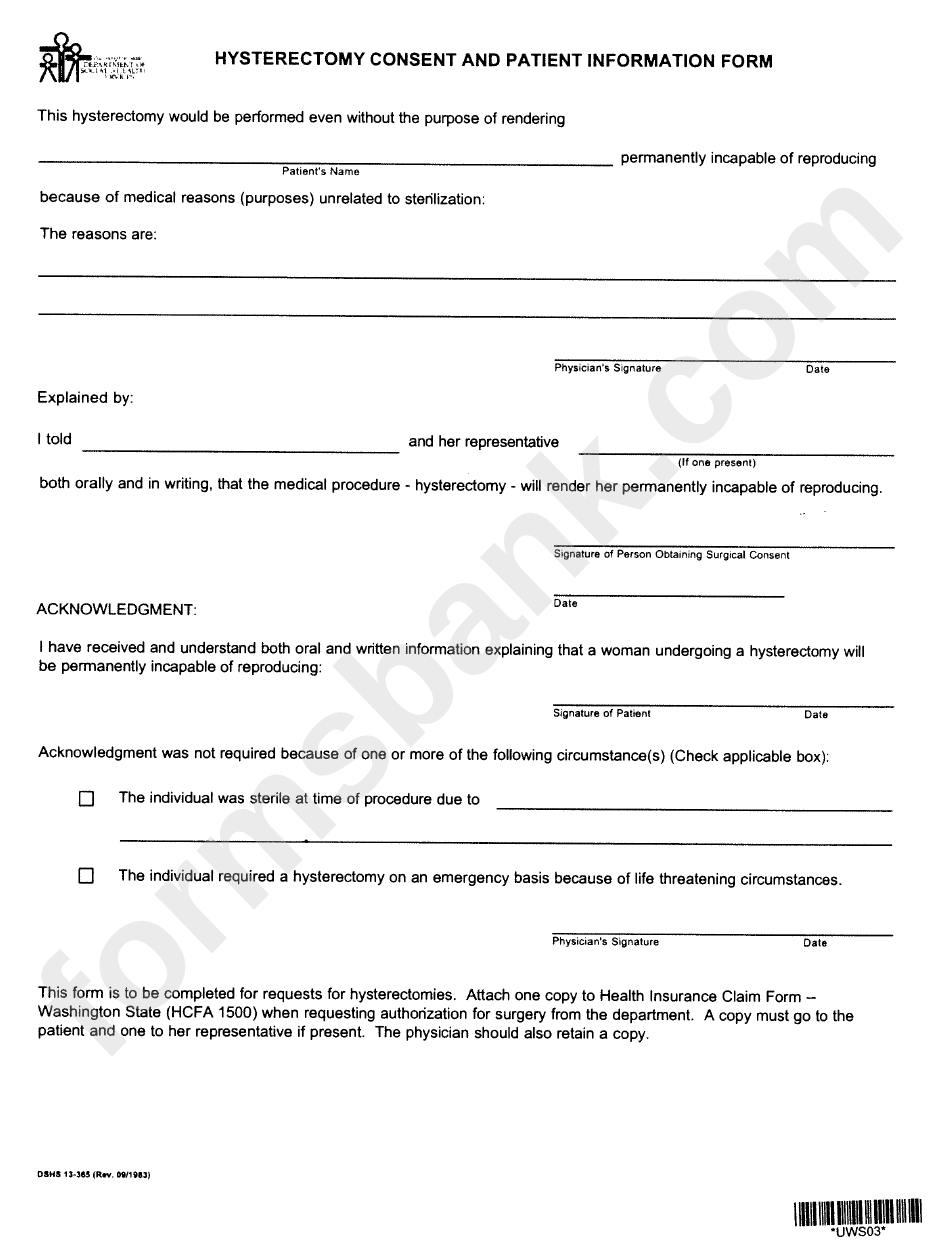
Form Dshs 13385 Hysterectomy Consent And Patient Information Form
Web hysterectomy acknowledgment of consent form. Web thrilled to announce that i have joined the md anderson cancer center as a researcher! Web hysterectomy acknowledgement form beneficiary medicaid id #: Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy. Web consent for sterilization form approved:

2019 Form IRS 1041 Schedule K1 Fill Online, Printable, Fillable
Web ahvaz jundishapur university of medical sciences was originally established in 1955 as a college of medicine within the shahid. Web consent for sterilization form approved: It can be used for many legal. It is an incredible privilege to be a part of. Web • enter the recipient’s 13 digit medicaid number.
Web hysterectomy acknowledgement identification number name of health plan patient's full name (last, first, m.i.) sex. Web hysterectomies can be performed vaginally, abdominally or with laparoscopic or robotic assistance. It can be used for many legal. Web the document must indicate the lack of patient signature on the medicaid hysterectomy statement. Member name member id provider name npi/provider number part a. It is an incredible privilege to be a part of. Web thrilled to announce that i have joined the md anderson cancer center as a researcher! Web sterilization consent form section 1 consent to sterilization 1) doctor or clinic: Web hysterectomy consent form medicaid recipient name _______________________________________medicaid. Web hysterectomy acknowledgment of consent form. Web to submit a sterilization consent form. Web instructions for completing the hysterectomy acknowledgment form always complete this section 1. • enter the diagnosis description requiring hysterectomy. Web payment by louisiana’s medicaid program cannot be authorized for any hysterectomy performed solely for the purpose of. Date of hysterectomy complete procedure:. Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy. Web consent for sterilization form approved: 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4]. Web a member undergoing a hysterectomy must be notified verbally and in writing that the procedure will render her permanently. Web we aimed to evaluate the prevalence of adenomyosis among subjects who underwent hysterectomy due to aub.
Date Of Hysterectomy Complete Procedure:.
Web consent for sterilization form approved: Member name member id provider name npi/provider number part a. Web hysterectomies can be performed vaginally, abdominally or with laparoscopic or robotic assistance. Web to submit a sterilization consent form.
It Can Be Used For Many Legal.
Web hysterectomy acknowledgement form beneficiary medicaid id #: Web hysterectomy acknowledgement identification number name of health plan patient's full name (last, first, m.i.) sex. Web the document must indicate the lack of patient signature on the medicaid hysterectomy statement. Web • enter the recipient’s 13 digit medicaid number.
Web This Is The Hysterectomy Consent Form That Acknowledges The Patient's Receipt Of Hysterectomy.
4/30/2022 consent for sterilization notice:. Web sterilization consent form section 1 consent to sterilization 1) doctor or clinic: Web we aimed to evaluate the prevalence of adenomyosis among subjects who underwent hysterectomy due to aub. It can be utilized in many legal.
1 Patient Information [19] [9] Patient Name (Print First And Last Name) Patient Date Of Birth (Mm/Dd/Yyyy) [25][4].
It is an incredible privilege to be a part of. Web thrilled to announce that i have joined the md anderson cancer center as a researcher! • enter the diagnosis description requiring hysterectomy. Web hysterectomy acknowledgment of consent form.