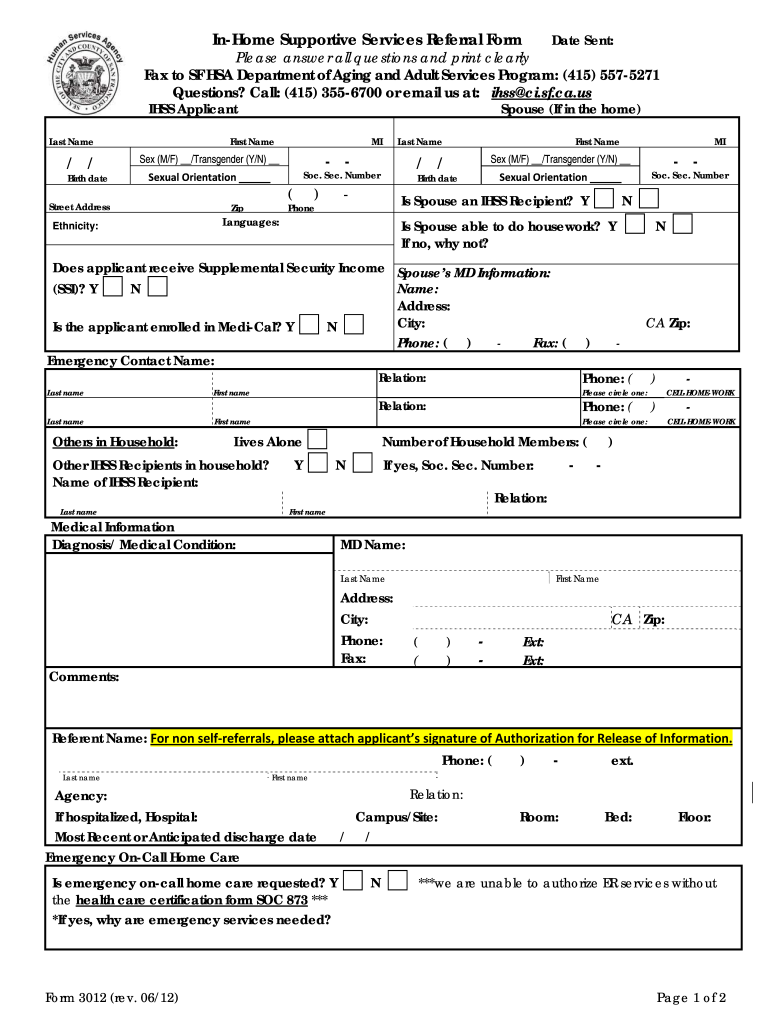
Ihss Authorized Representative Form - Web income supportive services referral form sf hsa department of disability and aging services program, fax: Web review the care plan and the physician attestation form upon initial enrollment, following any change in condition, and. Web denver, co employer est.: Cms, 7500 security boulevard, attn: Provide the weekly breakdown of days and hours: Sign online button or tick the preview image of the. Web right to have an authorized agent exercise your rights on your behalf. Cd's may be purchased by contacting the. Fill in the empty fields; Applicants can apply by phone, secure fax, and mail.
Form SOC839 Download Fillable PDF or Fill Online Inhome Supportive
Web review the care plan and the physician attestation form upon initial enrollment, following any change in condition, and. Web ihss, home health, and any other direct care services in the home. Web the ihss recipients (consumers) remain the employer for the purposes of hiring, firing,. We will require written proof of the agent’s. Web denver, co employer est.:

Alameda Alliance for Health Authorized Representative Form and
To get started on the document, use the fill camp; Sign online button or tick the preview image of the. Ihs recipient geworden an ihss addressee. We will require written proof of the agent’s. Fill in the empty fields;

Authorized Representative Form Sample Fill and Sign Printable
We will require written proof of the agent’s. Fill in the empty fields; Cms, 7500 security boulevard, attn: Notify the public authority of the names of. Web how to complete the ihss referral form on the web:
Form SOC839 Download Fillable PDF or Fill Online Inhome Supportive
Provide the weekly breakdown of days and hours: Web the ihss recipients (consumers) remain the employer for the purposes of hiring, firing,. Ihs recipient geworden an ihss addressee. Web and submit a completed health care certification form (soc 873). Sign online button or tick the preview image of the.

Form SOC838 Download Fillable PDF or Fill Online Inhome Supportive
Web ihss, home health, and any other direct care services in the home. Web and submit a completed health care certification form (soc 873). Web • consult with the client, authorized representative, or attendant in the event a medical issue arises. We will require written proof of the agent’s. Web how to complete the ihss referral form on the web:
Ihss Application Form Pdf Fill Online, Printable, Fillable, Blank
Ihs recipient geworden an ihss addressee. Web review the care plan and the physician attestation form upon initial enrollment, following any change in condition, and. Market street, sacramento, ca 95814, and is available to the public free of charge. Web conducts telephone intakes with ihss consumers and/or their authorized representatives, provides interview. Web job description complete initial and recertification assessments.
Form SOC839 Download Fillable PDF or Fill Online Inhome Supportive
Notify the public authority of the names of. Sign online button or tick the preview image of the. Cms, 7500 security boulevard, attn: Web conducts telephone intakes with ihss consumers and/or their authorized representatives, provides interview. Web form, please write to:
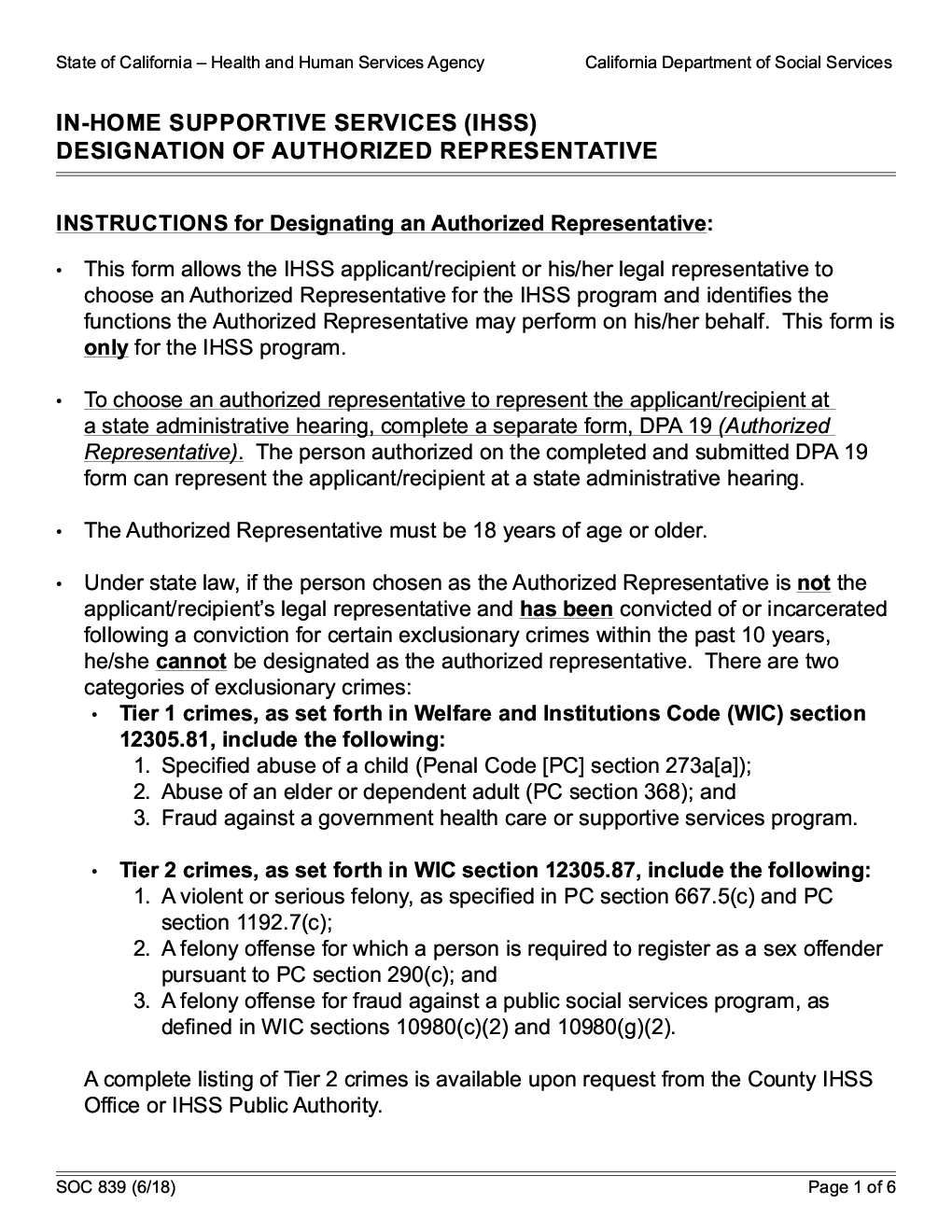
Form SOC 839. InHome Supportive Services (IHSS) Designation Of
Web review the care plan and the physician attestation form upon initial enrollment, following any change in condition, and. To get started on the document, use the fill camp; Applicants can apply by phone, secure fax, and mail. Web conducts telephone intakes with ihss consumers and/or their authorized representatives, provides interview. Sign online button or tick the preview image of.
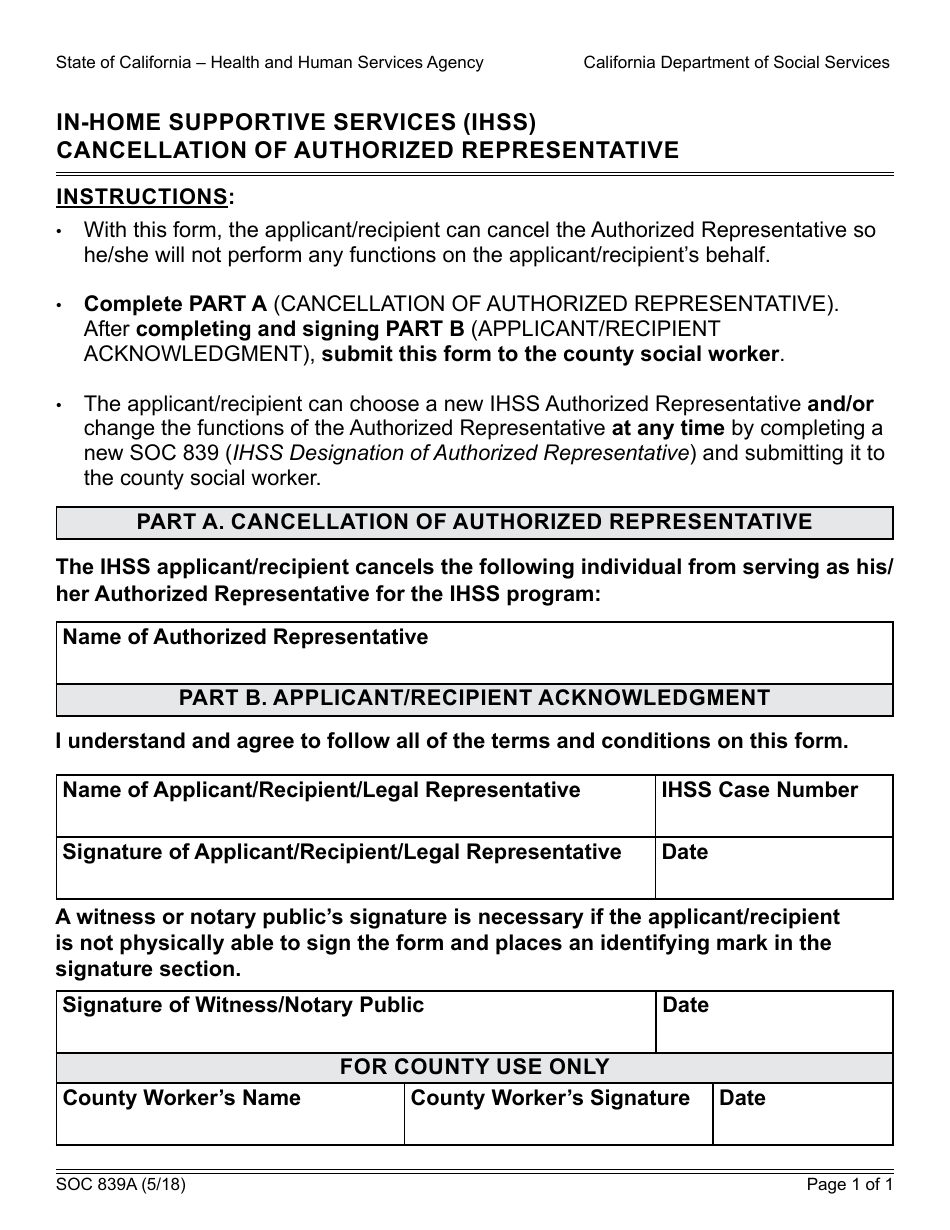
Form SOC839A Download Fillable PDF or Fill Online Inhome Supportive
Provide the weekly breakdown of days and hours: Web and submit a completed health care certification form (soc 873). Applicants can apply by phone, secure fax, and mail. Web the ihss recipients (consumers) remain the employer for the purposes of hiring, firing,. Live to homepage or in.
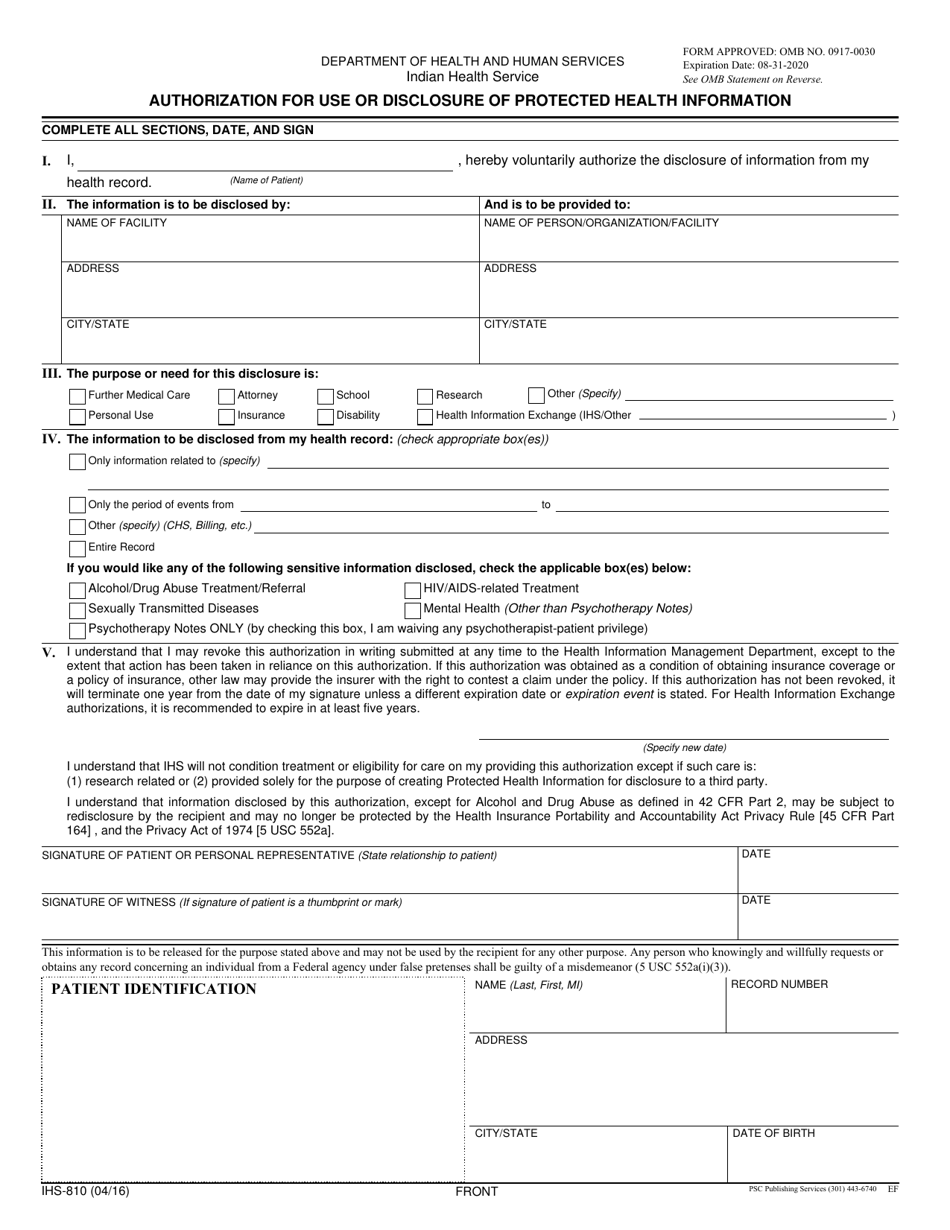
Form IHS810 Download Fillable PDF or Fill Online Authorization for Use
Web income supportive services referral form sf hsa department of disability and aging services program, fax: Provide the weekly breakdown of days and hours: Market street, sacramento, ca 95814, and is available to the public free of charge. Web ihss, home health, and any other direct care services in the home. Web the ihss recipients (consumers) remain the employer for.
Web income supportive services referral form sf hsa department of disability and aging services program, fax: Web review the care plan and the physician attestation form upon initial enrollment, following any change in condition, and. Cd's may be purchased by contacting the. Web the ihss recipients (consumers) remain the employer for the purposes of hiring, firing,. Provide the weekly breakdown of days and hours: We will require written proof of the agent’s. Web participants can designate an authorized representative (ar) to assist with tasks that are. Web conducts telephone intakes with ihss consumers and/or their authorized representatives, provides interview. Applicants can apply by phone, secure fax, and mail. Web find the ihss application form pdf you require. Fill in the empty fields; Sign online button or tick the preview image of the. Web how to complete the ihss referral form on the web: Web denver, co employer est.: Web right to have an authorized agent exercise your rights on your behalf. Web ihss, home health, and any other direct care services in the home. Web form, please write to: Web and submit a completed health care certification form (soc 873). Notify the public authority of the names of. Market street, sacramento, ca 95814, and is available to the public free of charge.
Provide The Weekly Breakdown Of Days And Hours:
Cms, 7500 security boulevard, attn: Web review the care plan and the physician attestation form upon initial enrollment, following any change in condition, and. Web how to complete the ihss referral form on the web: Sign online button or tick the preview image of the.
Live To Homepage Or In.
Applicants can apply by phone, secure fax, and mail. We will require written proof of the agent’s. Web income supportive services referral form sf hsa department of disability and aging services program, fax: Web participants can designate an authorized representative (ar) to assist with tasks that are.
Ihs Recipient Geworden An Ihss Addressee.
Web conducts telephone intakes with ihss consumers and/or their authorized representatives, provides interview. Web form, please write to: Cd's may be purchased by contacting the. Web • consult with the client, authorized representative, or attendant in the event a medical issue arises.
Web And Submit A Completed Health Care Certification Form (Soc 873).
To get started on the document, use the fill camp; Notify the public authority of the names of. Market street, sacramento, ca 95814, and is available to the public free of charge. Web the ihss recipients (consumers) remain the employer for the purposes of hiring, firing,.